Introduction
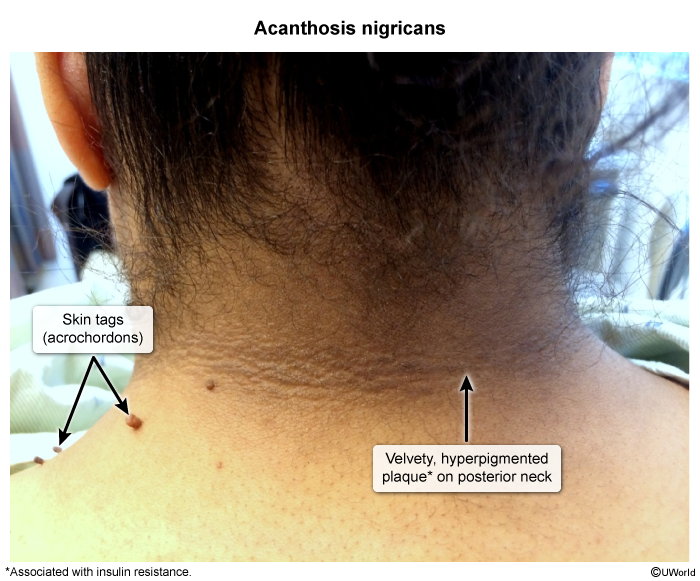
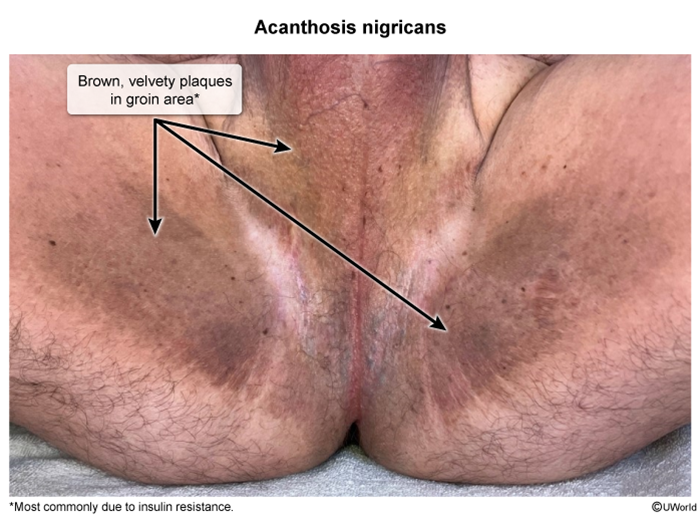
Acanthosis nigricans (AN) is a dermatologic condition characterized by hyperpigmented, velvety plaques, most commonly occurring in intertriginous areas. It is most often associated with insulin resistance but may also be linked to malignancy.
Pathophysiology
The exact mechanism underlying AN is not fully understood, but it is thought to result from keratinocyte and dermal fibroblast proliferation caused by increased activation of growth factor pathways. Insulin resistance plays a central role because hyperinsulinemia stimulates keratinocyte and fibroblast proliferation via insulin-like growth factor-1 (IGF-1) receptors. In malignancy-associated cases, tumor-secreted transforming growth factor-alpha (TGF-α) may induce similar epidermal hyperplasia.
Etiologies
AN may result from either benign or malignant causes. Benign causes can be acquired or inherited.
Benign causes
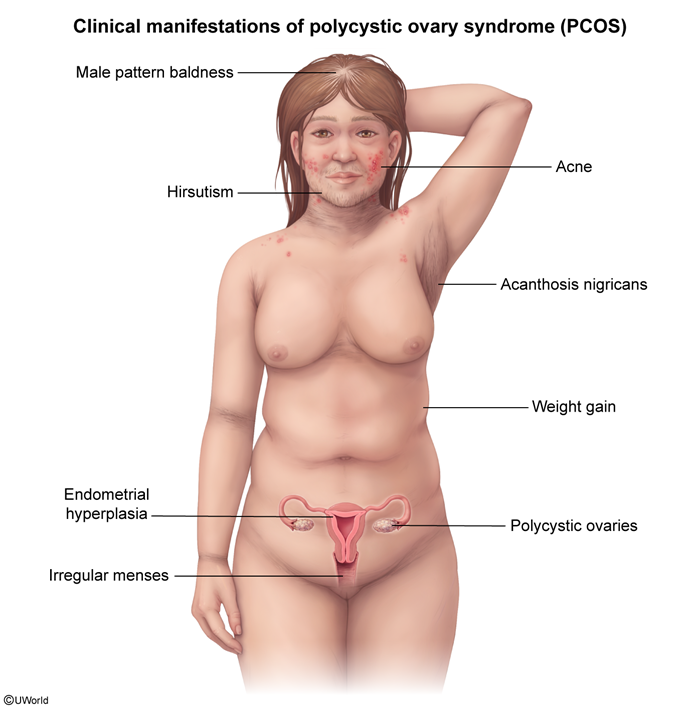
- Obesity and/or metabolic/endocrine disorders that are associated with insulin resistance (eg, type 2 diabetes mellitus, polycystic ovary syndrome, metabolic syndrome) are the most common etiologies of acquired AN.
- Medications that increase insulin resistance (eg, systemic glucocorticoid therapy, insulin therapy, oral contraceptive pills, niacin, protease inhibitors [eg, used to treat HIV and hepatitis C]) can similarly result in AN.
Rarely, inherited disorders (eg, associated with insulin or fibroblast growth factor receptor mutations) can also cause AN.
Malignant causes
Malignancies, particularly gastric adenocarcinomas, are associated with AN as a paraneoplastic marker. Other associated malignancies include cancers of the liver, lungs, and genitourinary system.
Pathology
Histologically, AN is characterized by the following
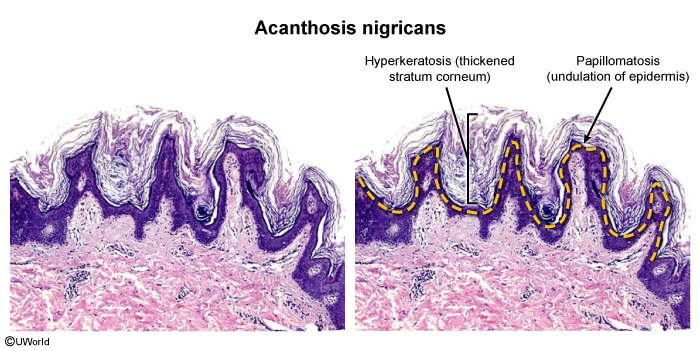
- Hyperkeratosis (thickening of the stratum corneum layer).
- Epidermal papillomatosis (undulating epidermal appearance with elongation of the dermal papilla and epidermal hyperplasia).
Increased melanin can be seen in the basal epidermal layer; however, hyperkeratosis is the main reason for AN's hyperpigmented appearance. Histologic examination does not distinguish between the different etiologies of AN and is therefore rarely needed for diagnosis.
Clinical presentation
AN classically presents with symmetric, hyperkeratotic, hyperpigmented plaques with a velvety texture in older children and adults who are overweight and insulin resistant. Lesions most commonly occur in the neck (posterior and lateral
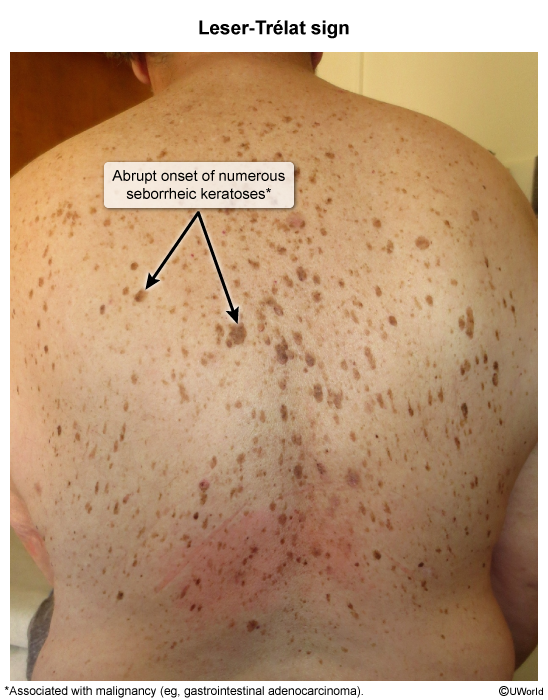
When associated with malignancy, AN typically presents in older adults with a new and rapid onset of AN without an identifiable cause (eg, obesity, hormone replacement therapy) or AN occurring at atypical locations (eg, palms, oral mucosa). In addition, unexplained weight loss or other cutaneous signs of cancer (eg, Leser-Trélat sign
Rarely, AN is seen during infancy and early childhood in association with genetic syndromes or familial forms. Patients generally have other syndromic features (eg, hypotonia, congenital heart disease as in Down syndrome) or a history of AN in first-degree relatives who are not obese or insulin resistant.
Diagnosis and evaluation
Diagnosis of AN is clinical, although a biopsy can be performed if the diagnosis is uncertain. Because of AN's association with systemic conditions, additional evaluation is recommended.
AN is associated with insulin resistance; therefore, patients should be screened for diabetes mellitus with fasting blood glucose and/or hemoglobin A1c measurement. In addition, women with signs and symptoms of polycystic ovarian syndrome (eg, hirsutism, oligomenorrhea, excessive uterine bleeding, acne) should be evaluated for AN
Older patients with features suggestive of malignancy-associated AN should undergo age-appropriate cancer screenings and additional diagnostic evaluations guided by symptoms. Because gastric adenocarcinoma is most frequently associated with AN, a consultation with a gastroenterologist should be considered.
Infants and young children with AN suggestive of genetic syndromes or hereditary familial disorders should be evaluated by a pediatric endocrinologist and a geneticist.
Differential diagnosis
- Hemochromatosis: Causes skin hyperpigmentation and diabetes mellitus due to iron overload; the hyperpigmentation is usually bronze and diffuse, not localized as in AN.
- Addison disease (primary adrenal insufficiency): Presents with diffuse hyperpigmentation that is more prominent in sun-exposed areas (eg, face, dorsal hands) and areas under pressure (eg, elbows, knees, bra lines) ( In contrast, AN presents with localized hyperpigmentation.
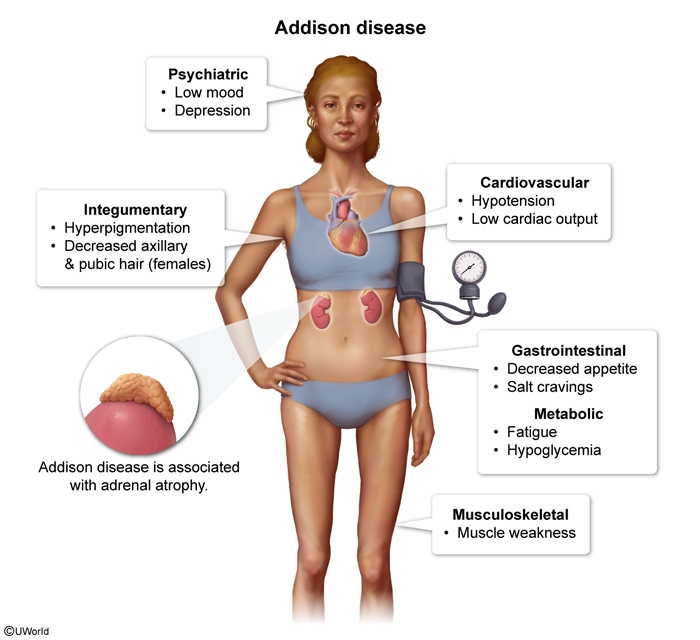 figure 2
figure 2 - Niacin deficiency (pellagra): Typically presents with a pigmented photosensitive dermatitis ( , erythematous tongue, diarrhea, vomiting, and neurologic symptoms (eg, insomnia, dementia, confusion). It affects patients with malabsorption (eg, heavy alcohol use, inflammatory bowel disease, bariatric surgery status) or limited oral intake (eg, anorexia nervosa, residence in resource-limited settings), none of which are risk factors for AN.
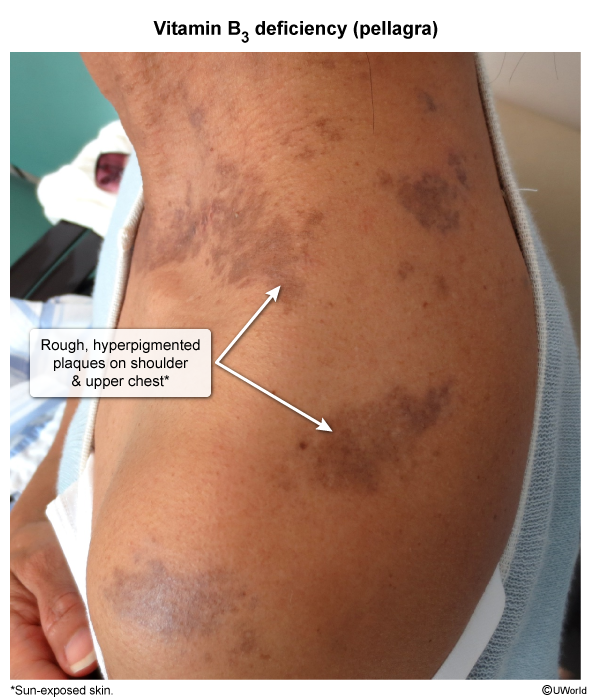 image 5
image 5
Other rare dermatologic disorders are also included in the differential diagnosis.
Management
Management of AN focuses on the correction of underlying conditions, which often leads to the resolution of AN. Patients with obesity should be counseled on weight loss. Individuals with medication-induced AN should discontinue the offending drug, if possible. Patients with malignancy-related AN should be treated for the underlying malignancy.
Dermatologic therapies can also be used to expedite the resolution of AN. For AN covering a small area, topical retinoid therapy (eg, tretinoin, adapalene), topical keratolytics (eg, ammonium lactate, urea), or topical vitamin D analogues (eg, calcipotriene) can be used to reduce hyperkeratosis or inhibit keratinocyte proliferation. For widespread AN, systemic retinoids (eg, isotretinoin, acitretin) may be considered.
Complications
Although AN is harmless, the psychosocial impact due to its cosmetic effects can be significant.
Prognosis
By itself, AN is benign and tends to persist chronically. Correcting the underlying cause and/or using dermatologic therapy may result in the resolution of AN.
Summary
Acanthosis nigricans is a dermatologic condition characterized by hyperpigmented, velvety plaques that occur in the axillae, groin, and neck. It most commonly presents in overweight children and adults who are insulin resistant; rarely, it may present in older adults with malignancy (eg, gastric adenocarcinoma). Acanthosis nigricans is thought to result from keratinocyte and dermal fibroblast proliferation due to increased activation of growth factor pathways. Diagnosis is clinical, and evaluation typically includes screening for diabetes mellitus due to AN's association with insulin resistance. In older patients with weight loss and new-onset, rapidly progressing AN, an evaluation for occult malignancy is indicated. Management focuses on treating the underlying conditions (eg, weight loss for overweight patients), which typically leads to the resolution of AN. If desired for cosmetic reasons, topical therapies (eg, retinoid, ammonium lactate, urea) can be used to expedite resolution.