The maintenance of acid-base balance is crucial for normal cellular function and overall homeostasis. The body tightly regulates concentrations of hydrogen (H+), bicarbonate (HCO3−), and partial pressure of carbon dioxide (PaCO2) through buffering systems, respiratory control, and renal compensatory mechanisms. These systems work together to keep the blood pH between 7.35 and 7.45. However, various metabolic and respiratory insults can disrupt these regulatory mechanisms and result in acid-base disorders. These disorders are broadly categorized based on blood pH, with acidemia present for pH <7.35 and alkalemia for pH >7.45.
Although the terms are sometimes used loosely, metabolic or respiratory acidosis or alkalosis represent individual processes that contribute to the overall acid-base status, which should be described using acidemia or alkalemia (eg, a metabolic acidosis could be present, but the overall acid-base status could be normal due to the buffering systems.
Pathophysiology and etiologies
Acid-base disorders are characterized by a primary disturbance in the blood concentration of HCO3− (metabolic) and/or PaCO2 (respiratory. In response to these disturbances, compensatory mechanisms attempt to restore pH to a normal level (although they cannot fully normalize pH. In some cases, there can be more than one primary metabolic or respiratory component (ie, mixed disorder. Acid-base disorders are categorized into 4 types:
Metabolic acidosis
Metabolic alkalosis
Respiratory acidosis
Respiratory alkalosis
Metabolic acidosis
A primary decrease in HCO3– lowers blood pH. Mechanisms include:
Increased acid production
Conditions such as lactic acidosis (eg, hypoperfusion, sepsis), ketoacidosis (eg, insulin deficiency), and ingestion of toxins (eg, toxic alcohols, salicylates) result in the accumulation of organic acids.
Loss of HCO3−
Gastrointestinal losses (eg, bicarbonate-rich fluid loss in diarrhea or fistulas) or type 2 (proximal) renal tubular acidosis (RTA) lead to HCO3− wasting.
Decreased acid excretion
Chronic kidney disease and type 1 (distal) and type 4 RTA reduce the kidneys' ability to excrete H+.
Metabolic alkalosis
A primary increase in HCO3− raises blood pH. Mechanisms include:
Loss of H+
Prolonged vomiting or nasogastric suction removes gastric acid, containing both H+ and chloride (Cl−) ions. Excess mineralocorticoid activity increases H+ secretion in the distal nephron.
Increased HCO3− retention
Diuretics and hypokalemia promote renal HCO3− reabsorption (eg, maintenance of electrochemical balance.
HCO3− administration
Excessive intake of HCO3− (eg, antacids) can directly increase serum HCO3− levels (eg, milk-alkali syndrome.
Respiratory acidosis
A primary increase in PaCO2 (due to hypoventilation) lowers blood pH. Causes of hypoventilation include:
"Won't breathe" (central causes)
These represent central causes affecting the brainstem and cortex
Drug overdose (opioids, benzodiazepines), central nervous system lesions (eg, stroke, trauma), and infections (eg, encephalitis) cause central respiratory depression.
"Can't breathe" (peripheral causes)
These represent peripheral causes affecting respiratory muscles, thoracic cage, and lungs.
Airway obstruction (eg, chronic obstructive pulmonary disease, asthma) or lung parenchyma damage (eg, restrictive lung disease) prevent appropriate air exchange.
Respiratory alkalosis
A primary decrease in PaCO2 (due to hyperventilation) raises blood pH. Increased pH enhances binding of calcium to albumin, lowering ionized calcium levels with potential symptoms (eg, paresthesias, carpopedal spasm, tetany. Causes of hyperventilation include:
Respiratory stimulation (central): Anxiety, pain, fever, salicylate toxicity, high progesterone levels (eg, pregnancy, cirrhosis), and hypoxemia (eg, high altitude)
Pulmonary causes: Acute pulmonary embolism or pneumonia can cause hyperventilation due to ventilation/perfusion mismatch.
Evaluation
Arterial blood gas analysis
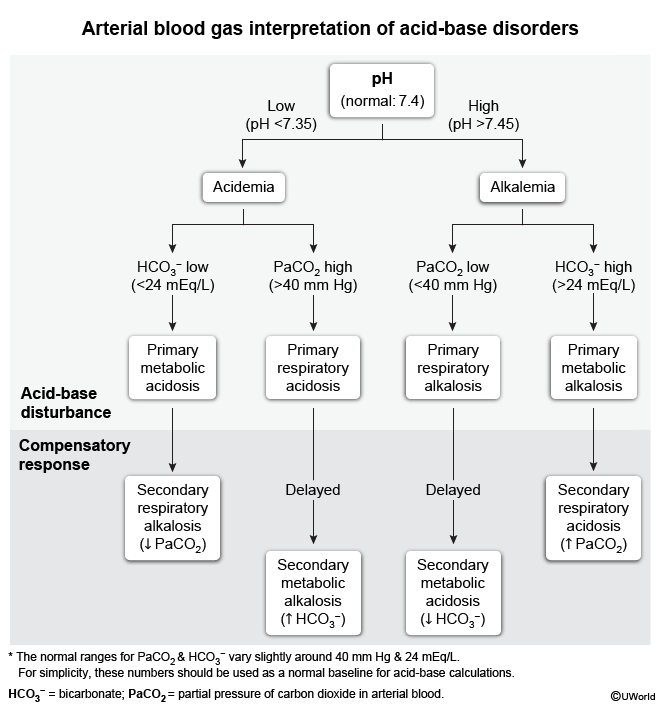
Evaluation of acid-base disorders begins with an arterial blood gas (ABG) test and a basic metabolic panel (BMP)
figure 1. Analysis is best performed in a stepwise fashion:
Assess pH: Determine the patient's overall acid-base status based on the ABG test; acidemia is present if pH <7.35 and alkalemia is present if pH >7.45.
Determine the primary disorder: Analyze the metabolic component (serum HCO3−, normal: 24 mEq/L) and respiratory component (PaCO2, normal: 40 mm Hg. (Measured HCO3− from a BMP is preferred over the calculated value obtained from blood gas analysis given the potential for assay interference.) The component shifted in the direction that explains the change in pH represents the primary disorder.
Metabolic acidosis: ↓ pH, ↓ HCO3−
Metabolic alkalosis: ↑ pH, ↑ HCO3−
Respiratory acidosis: ↓ pH, ↑ PaCO2
Respiratory alkalosis: ↑ pH, ↓ PaCO2
Evaluate compensation mechanisms: Primary metabolic disorders are quickly compensated by changes in alveolar ventilation. Compensation for primary respiratory disorders is minimal for acute acid-base disorders and reaches full compensation after approximately 72 hours. If PaCO2 or HCO3− levels are within the expected range ), the response is considered appropriate (ie, secondary acid-base compensation. If these values are different than expected, an additional primary acid-base disorder is present:
In primary metabolic disorders, higher than expected PaCO2 indicates an additional primary respiratory acidosis, and lower than expected PaCO2 indicates an additional respiratory alkalosis.
In primary respiratory disorders, higher than expected HCO3− indicates an additional primary metabolic alkalosis, and lower than expected HCO3− indicates an additional metabolic acidosis.
Anion gap and non–anion gap metabolic acidosis
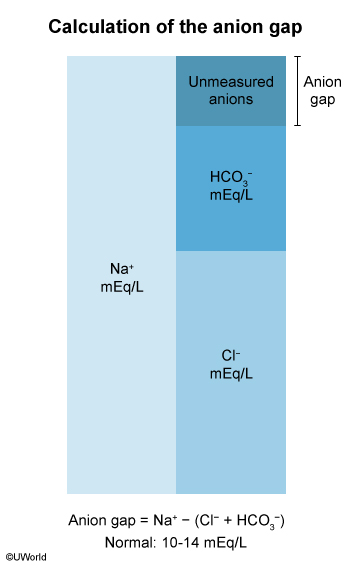
The anion gap (AG) should be calculated, especially in patients with metabolic acidosis. The AG consists of unmeasured anions normally present in the serum and is equal to Na+ − (Cl⁻ + HCO3−) (normal: 10-14 mEq/L)
figure 2. Metabolic acidosis can then be subclassified into:
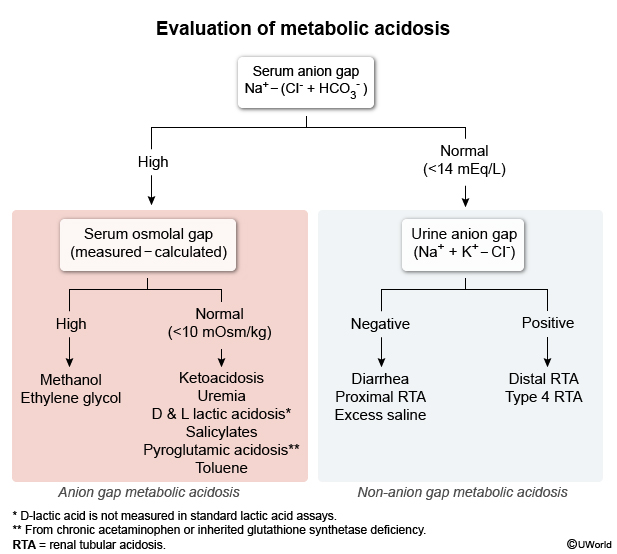
Anion gap metabolic acidosis (AGMA): Causes can be recalled using the mnemonic GOLDMARK:
Glycols: Ethylene glycol (converted to toxic glycolic and oxalic acids, cause renal injury), propylene glycol
Oxoproline: Pyroglutamic acidosis from chronic acetaminophen use
L-lactate: Classic lactic acidosis from various causes such as hypoperfusion, sepsis, or hypoxia
D-lactate: Rare lactic acidosis seen in short bowel syndrome or small intestinal bacterial overgrowth
Methanol: Converted to the toxic formaldehyde and formic acid (retinal injury)
Aspirin (salicylates): Overdose leads to metabolic acidosis (with a respiratory alkalosis component)
Renal failure: Causing accumulation of organic acids (eg, sulfates)
Ketoacidosis: Diabetic, alcoholic, or starvation
Normal anion gap metabolic acidosis (NAGMA): Also known as hyperchloremic metabolic acidosis; may be caused by:
Diarrhea: Loss of bicarbonate-rich fluid in stool
RTA: Accumulation of inorganic acids (H+ that do not elevate the anion gap
Excess normal saline: Hyperchloremia promoting HCO3– excretion (via the pendrin chloride/HCO3− exchanger)
The differential diagnosis for AGMA and NAGMA can be narrowed by calculating the serum osmolal gap and urine anion gap, respectively
figure 3.
Urinary chloride for metabolic alkalosis
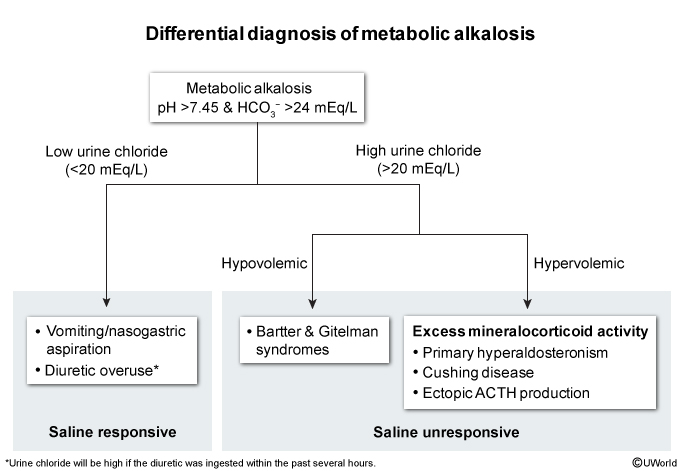
Metabolic alkalosis etiologies can be differentiated by urine Cl− measurements
figure 4 ):
Low urine Cl− (<20 mEq/L) reflects the kidneys' attempt to increase Cl− reabsorption in volume-depleted patients, such as those with diuretic overuse or vomiting (ie, saline responsive metabolic alkalosis.
High urine Cl− (>20 mEq/L) reflects renal wasting of Cl− (ie, saline unresponsive metabolic alkalosis. Hypervolemic etiologies include excess mineralocorticoid activity (eg, primary hyperaldosteronism. Hypovolemic etiologies include disordered renal handling of Na+ and Cl− (ie, Bartter and Gitelman syndromes.
Respiratory acidosis versus alkalosis
Respiratory acidosis and alkalosis can be further evaluated with pulmonary function testing (differentiates obstructive vs restrictive causes), chest x-ray (eg, pneumonia), D-dimer test and CT pulmonary angiography (eg, pulmonary embolism), and evaluation for anxiety disorders.
Mixed acid-base disorders
The coexistence of ≥2 primary acid-base disorders results in a mixed acid-base disorder
.
Most mixed disorders can be identified with relative ease in the presence of a very low or high pH (PaCO2 or HCO3− move in opposite directions) or a near normal pH (PaCO2 or HCO3− move in the same direction.
However, mixed metabolic acidosis and alkalosis can be subtle given that pH, PaCO2, and HCO3− are nearly normal due to the offsetting of underlying disturbances. For example, in diabetic ketoacidosis (DKA) with severe vomiting, acid accumulation pushes HCO3− downward with a compensatory decrease in PaCO2, while vomiting drives HCO3− upward with a compensatory increase in PaCO2.
The delta-delta ratio (ΔAG/ΔHCO3−) can help identify another metabolic disorder in addition to AGMA; ΔAG = patient's AG − 10 (normal anion gap) and ΔHCO3− = 24 (normal HCO3−) - patient's HCO3−.
A ratio >2 suggests an additional metabolic alkalosis (ie, HCO3− being pulled in opposite directions decreases the denominator), as in the example of DKA with severe vomiting.
A ratio <1 suggests an NAGMA coexisting with AGMA, as in diarrheal illness (NAGMA) precipitating DKA (AGMA.
Management
Management of acid-base disorders focuses on treating the underlying cause, which will restore homeostasis in most cases. In some cases, directly treating the acid-base disturbance is necessary (eg, bicarbonate infusion, renal replacement therapy.
Metabolic acidosis
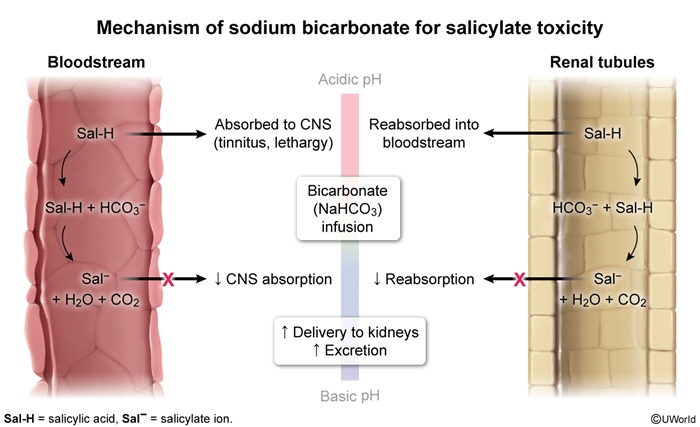
AGMA typically does not require bicarbonate infusion because bicarbonate does not address the underlying driver of acidosis (accumulation of organic acids) and may worsen acidosis by generating CO2; a notable exception is salicylate poisoning, in which bicarbonate is administered to alkalize the urine, promoting salicylate excretion ( figure 5.
Glycol and methanol poisonings are treated with fomepizole (which inhibits alcohol dehydrogenase) to reduce toxic metabolite accumulation; hemodialysis is performed in severe cases.
Classic lactic acidosis (L-lactate) requires optimizing tissue perfusion, including intravenous fluids, antibiotics, and vasopressors (sepsis); inotropes or mechanical circulatory support (cardiogenic shock); and surgery or revascularization (bowel ischemia.
Diabetic and alcohol ketoacidosis are managed with insulin/intravenous fluids and thiamine/dextrose, respectively.
In NAGMA, bicarbonate infusion can be used to directly replace lost HCO3− (eg, from diarrhea.
Type 1 (distal) RTA is treated with oral bicarbonate or citrate, whereas type 2 (proximal) RTA is managed with high-dose oral bicarbonate and thiazide diuretics (to reduce bicarbonate loss.
Type 4 RTA (hypoaldosteronism) requires the administration of a mineralocorticoid (eg, fludrocortisone.
Metabolic alkalosis
Saline-responsive metabolic alkalosis due to volume depletion can be corrected with isotonic saline to replete Cl− while addressing the underlying cause (eg, antiemetics.
Saline-resistant metabolic alkalosis is managed with a mineralocorticoid receptor antagonist (eg, spironolactone) for primary hyperaldosteronism or surgical resection for aldosterone-producing adenomas.
Respiratory acidosis and alkalosis
Respiratory acidosis treatment primarily focuses on improving ventilation through noninvasive or invasive mechanical ventilation, depending on the severity and underlying cause. Pharmacologic therapies such as bronchodilators, corticosteroids, and naloxone are often necessary.
Respiratory alkalosis is treated by addressing the underlying cause (eg, anxiolytics, analgesics.
Summary
Acid-base disorders arise from disturbances in the body's buffering systems, respiratory control, and renal compensatory mechanisms. Arterial blood gas and serum chemistries are used to determine the primary disorder, which can be classified as metabolic acidosis (↓ pH, ↓ HCO3−), metabolic alkalosis (↑ pH, ↑ HCO3−), respiratory acidosis (↓ pH, ↑ PaCO2), or respiratory alkalosis (↑ pH, ↓ PaCO2.
In metabolic acidosis, calculating the anion gap helps differentiate between causes such as lactic acidosis, ketoacidosis, and toxic ingestions (high anion gap) and conditions such as diarrhea, renal tubular acidosis, and excessive normal saline administration (normal anion gap. In metabolic alkalosis, measuring urinary Cl⁻ distinguishes between saline-responsive etiologies such as volume depletion (urine Cl⁻ <20 mEq/L) and saline-resistant etiologies such as primary hyperaldosteronism (urine Cl⁻ >20 mEq/L. Calculations are used to determine the presence of appropriate compensation (ie, secondary compensation) or mixed primary disorders.
Management primarily focuses on treating the underlying cause, allowing homeostasis to be restored. In some cases, direct intervention to correct the acid-base disturbance may be necessary; bicarbonate infusion may be given to replace lost HCO3− from diarrhea in normal anion gap metabolic acidosis and toxic ingestions/renal failure may necessitate renal replacement therapy.