Annular pancreas is a rare congenital anomaly in which a ring of pancreatic tissue encircles the duodenum. Patients with annular pancreas are often asymptomatic but may have signs of duodenal obstruction (eg, abdominal distension, emesis.
Pathophysiology and risk factors
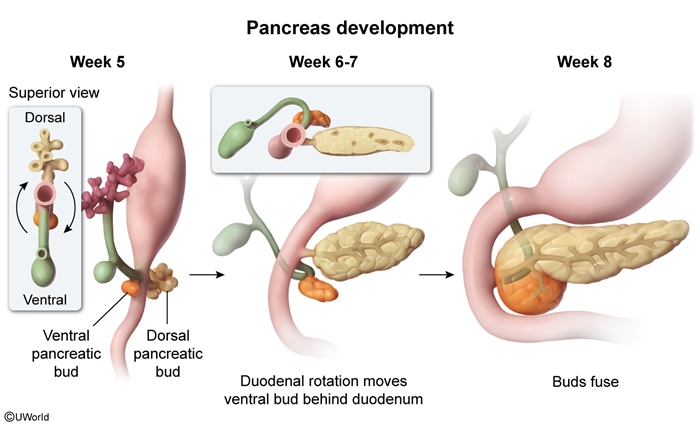
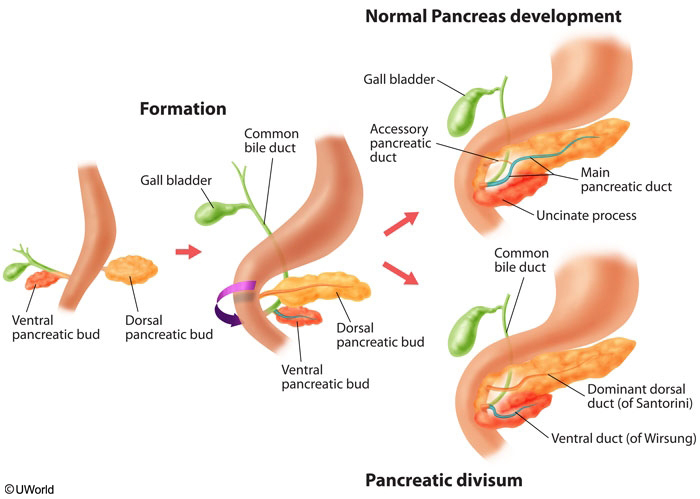
Pancreatic development is a complex process that involves the formation, rotation, and fusion of the dorsal and ventral pancreatic buds, which are foregut derivatives
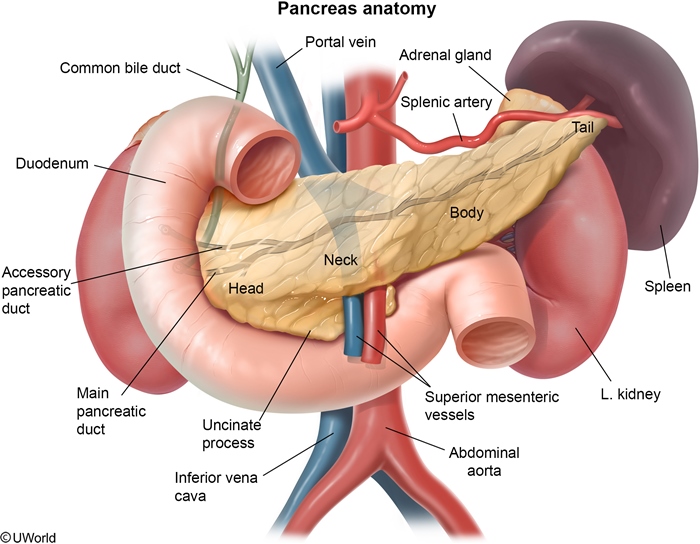
figure 1. The ventral pancreatic bud gives rise to the uncinate process of the pancreatic head and the main pancreatic duct ( figure 2. The dorsal pancreatic bud gives rise to the remainder of the pancreatic head as well as the tail and body.
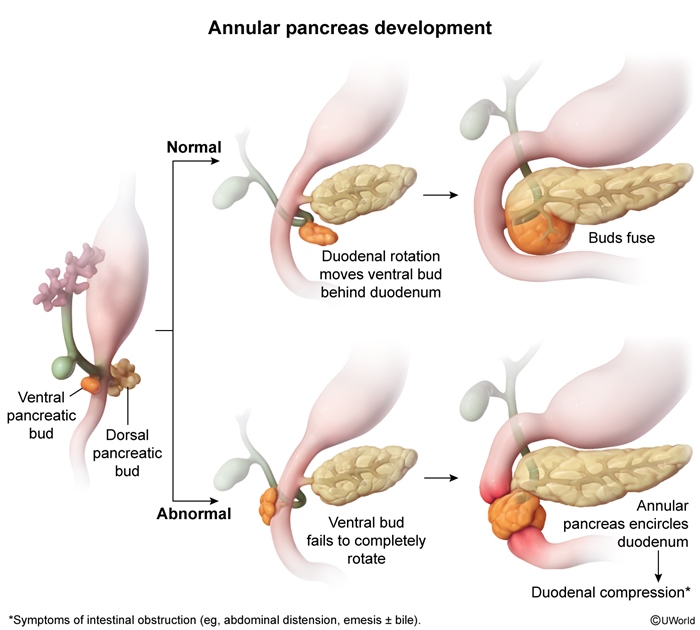
Normally, the ventral pancreatic bud rotates behind the duodenum and fuses with the dorsal pancreatic bud by the 8th week of gestation. Annular pancreas develops when the ventral pancreatic bud fails to rotate completely
figure 3 ), resulting in a partial or complete ring of pancreatic tissue that encircles the second portion of the duodenum, thereby causing varying degrees of obstruction. Histologically, the annular pancreas comprises normal pancreatic tissue, including both exocrine and endocrine components.
Although the exact causes are not well defined, there is a higher incidence of annular pancreas in individuals with trisomy 21 (Down syndrome) and other congenital anomalies involving the gastrointestinal (GI) tract (eg, duodenal atresia, Meckel diverticulum.
Clinical presentation
The majority of patients with annular pancreas are asymptomatic. However, in some patients, the circumferential pancreatic tissue can compress the duodenal lumen, causing obstruction that can be either proximal (nonbilious emesis) or distal (bilious emesis) to the major duodenal papilla
figure 4. Annular pancreas can also obstruct pancreatic drainage, causing pancreatitis.
Of note, the age at symptom onset varies depending on the severity of obstruction; complete obstruction often presents shortly after birth, similar to duodenal atresia. Partial obstruction may present in adulthood with nonspecific symptoms (eg, chronic abdominal pain, postprandial fullness, nausea.
Diagnosis
In patients with suspected annular pancreas, diagnostic evaluation includes:
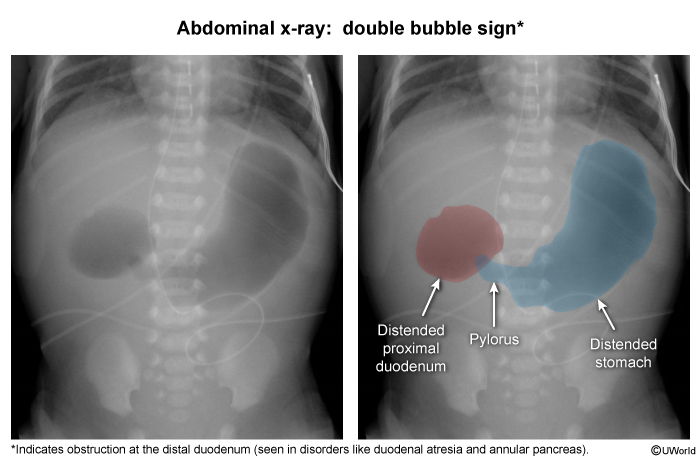
Abdominal radiography may show a double bubble sign with trapped air in the stomach and proximal duodenum; it is a nonspecific finding indicative of obstruction in the distal duodenum (it can also be seen in duodenal atresia and midgut volvulus) ( image 1.
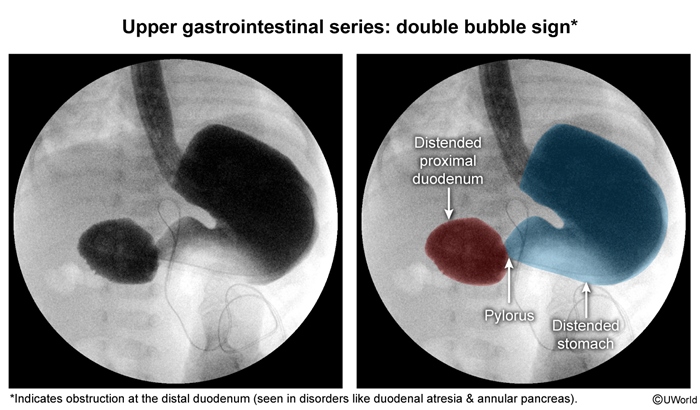
An upper GI series may demonstrate constriction of the second part of the duodenum with proximal dilation ( image 2 ), although this is not specific for annular pancreas.
A CT scan provides detailed anatomical visualization, showing a ring of pancreatic tissue encircling the duodenum.
MR cholangiopancreatography is noninvasive imaging that visualizes the pancreatic ducts and annular ring; it may be performed if prior imaging is inconclusive.
Of note, if abdominal radiography in infants is consistent with duodenal obstruction, patients usually proceed to surgery, where the etiology of the obstruction can be confirmed.
Laboratory evaluation is generally not diagnostic but may be obtained if electrolyte derangements are suspected due to recurrent emesis. Pancreatic enzyme levels may be elevated if pancreatitis is present.
Differential diagnosis
The differential diagnosis for annular pancreas includes other congenital anomalies that may cause duodenal obstruction, including:
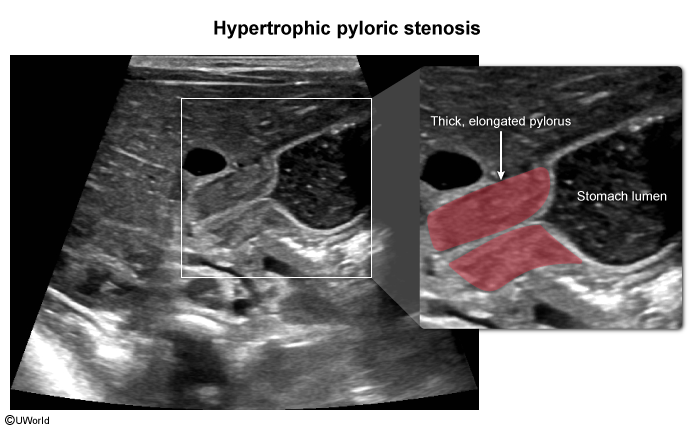
Pyloric stenosis ( image 3 ): classically presents in infancy with projectile, nonbilious (obstruction typically occurs proximal to the major duodenal papilla) emesis and a palpable olive-shaped mass on examination. Because the obstruction is at the level of the pylorus, there is no double bubble sign. Abdominal ultrasonography reveals a thickened and elongated pylorus.
Duodenal atresia: is a congenital defect in which a segment of the duodenal lumen is completely obstructed; patients classically have feeding intolerance, bilious emesis, and mild abdominal distension. Similar to annular pancreas, imaging reveals a double bubble sign with trapped air in the stomach and proximal duodenum.
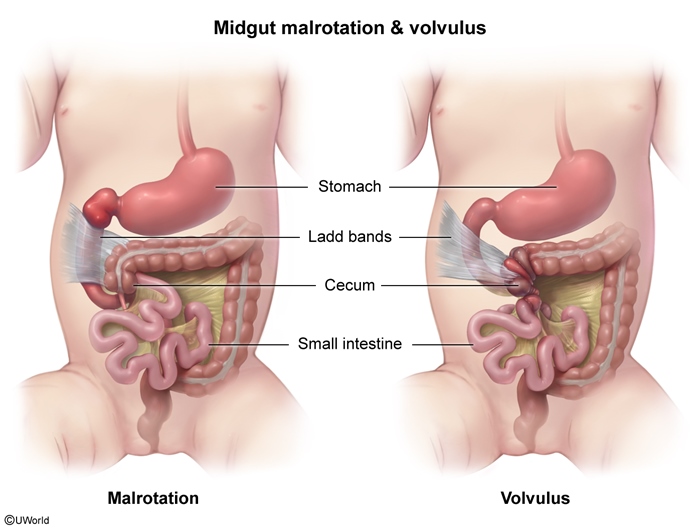
Midgut malrotation with volvulus ( figure 5 ): presents with bilious emesis and abdominal pain. Contrast imaging reveals intestines in the right side of the abdomen.
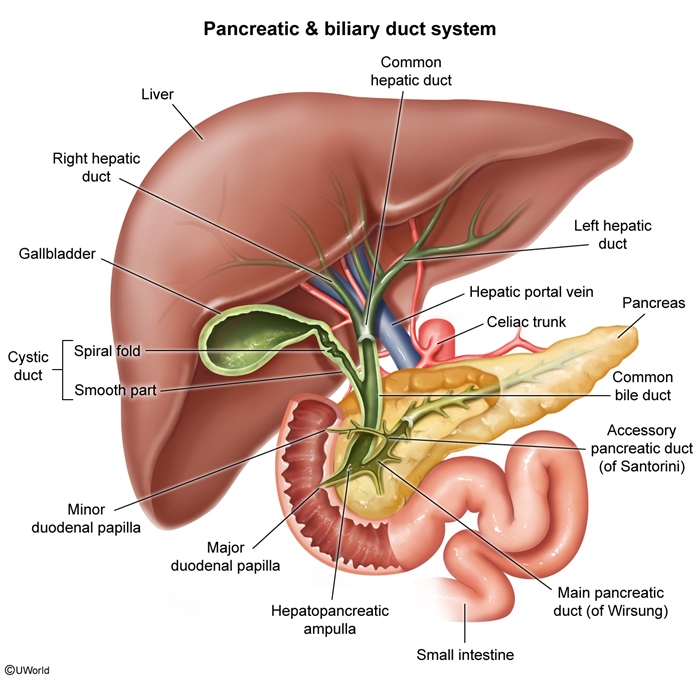
Pancreatic divisum, another pancreatic congenital anomaly, results from failed fusion of the dorsal and ventral pancreatic ducts
figure 6. However, because the pancreatic buds fuse normally, there is no duodenal obstruction. Patients are usually asymptomatic, but some may develop recurrent pancreatitis.
Management
In patients who have signs of duodenal obstruction, management involves surgical intervention to bypass the obstructing tissue. This can be accomplished via the following procedures:
Duodenoduodenostomy (most common surgical procedure) creates a bypass around the obstruction to the distal duodenum.
Duodenojejunostomy or gastrojejunostomy creates a bypass to the jejunum (more commonly performed in adults.
Resection of the obstructing pancreatic tissue is generally avoided due to the risk for complications (eg, pancreatitis, fistula formation.
Summary
Annular pancreas is a rare congenital anomaly in which a ring of pancreatic tissue encircles the duodenum. Patients with annular pancreas are often asymptomatic but may have signs of duodenal obstruction (eg, abdominal distension, emesis. Management of symptomatic patients involves surgical intervention (eg, duodenoduodenostomy) to bypass the site of obstruction.